
James, a 64-year-old African-American male with Stage 4 chronic kidney disease, was told by his nephrologist to choose a treatment plan for end-stage kidney disease (ESKD). James knew he needs some form of treatment to survive, so he attended a kidney education class to learn more about which treatment would be the best for him. He learned that there are four treatment options: 1) hemodialysis; 2) peritoneal dialysis; 3) kidney transplantation; or 4) palliative care. The following will provide a brief overview of his options he learned about.
 Hemodialysis
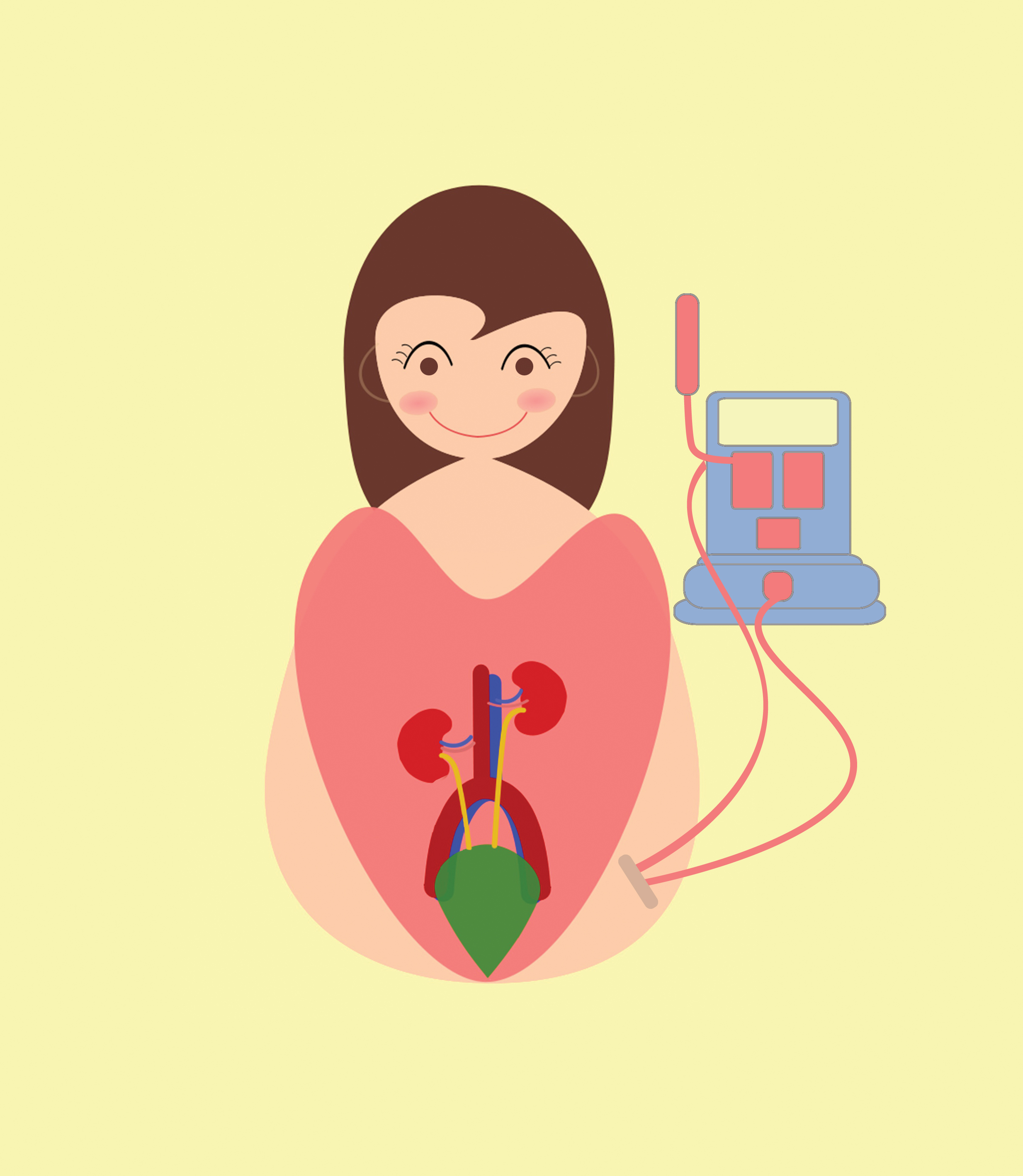
Hemodialysis
Hemodialysis (HD) requires a machine and a filter called an artificial kidney or dialyzer. The dialyzer has two parts: one with fibers that your blood flows through and one with the washing fluid (dialysate). A thin membrane that separates these two parts allows removal of waste products (e.g. urea, creatinine) and extra electrolytes (e.g. potassium, sodium) and fluids from your blood, but will not let protein or red blood cells come through. You need to have a hemodialysis access, and the best one is an arteriovenous fistula (AVF) in your arm, which is created in minor surgery. HD can be done at home or in a dialysis center. In-center HD is usually three times a week for 4 hours each time. One type of home HD is performed by a nurse or technician similar to in-center HD. The other type of home HD is done by you along with your designated care partner. This type of HD is done about five times a week using a machine that does not require an external water treatment system. The last type of home HD is called nocturnal HD; it occurs while you sleep for about six to eight hours every other night or six times per week.
 Peritoneal Dialysis
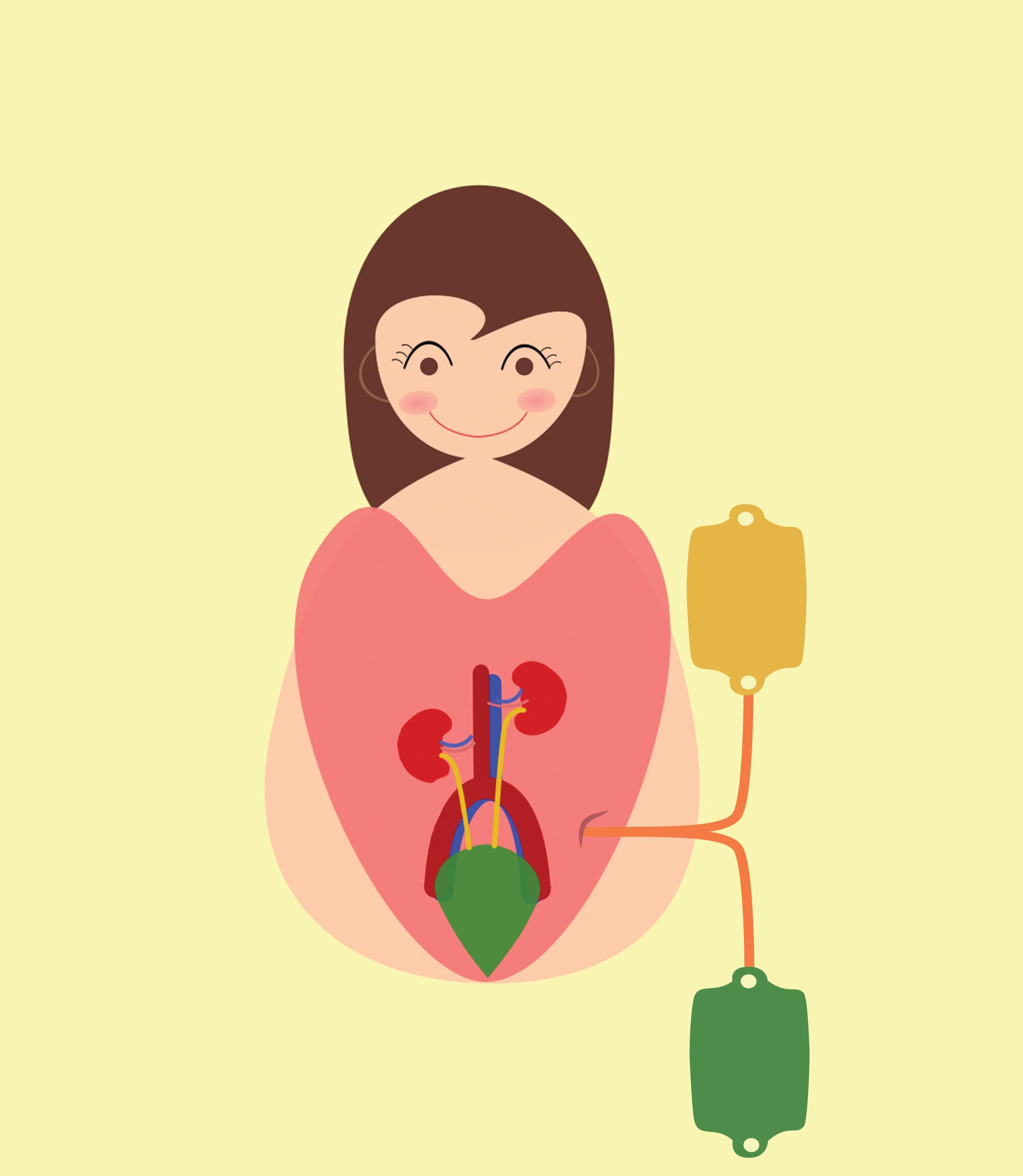
Peritoneal Dialysis
In peritoneal dialysis the lining of your own belly acts as a filter similar to the one in HD. However, rather than having the surgeon create an AVF, the surgeon will place a catheter (soft plastic tube) into your belly. A sterile solution (dialysate) will be placed in your belly either by using a machine (automated PD [APD]) or by raising the bag of solution to shoulder height to cause it to flow in by gravity (continues ambulatory PD [CAPD]). The fluid will be placed in your belly for a prescribed time and then drained and replaced with new solution (called an exchange). You don’t use a machine for CAPD but will have to perform it about four times a day, seven days a week. APD uses a machine to perform the exchanges while you sleep at night (seven nights a week).
![]() Kidney Transplant
Kidney Transplant
A kidney transplant is not a cure, but rather another treatment option. It requires surgery, and placement of a new kidney from a living related donor, non-related living donor or deceased donor, on the right or left side of your lower abdomen. The surgery usually takes about three to five hours. To be considered for a transplant, your nephrologist will refer you to a transplant center for evaluation. Any potential living donor would have to undergo an evaluation as well. You will have to take medications to reduce the chance of rejection. Rejection is when your body’s immune system considers the organ from another person as foreign and begins to attack it. You will have to take antirejection medications to help prevent this from occurring. The transplant team will carefully monitor you, especially during the first year after the transplant, to try to prevent rejection. In the event of rejection, you will have another opportunity to be evaluated for a second transplant.
Palliative Care
Some people may decide they don’t want one of the aforementioned treatments, and instead choose palliative care. Palliative care is specialized medical care for people with advanced chronic disease such as ESKD. The goal of care is to manage any symptoms someone may be experiencing due to advanced disease, and to improve quality of life for the individual and the family. When death is anticipated in 6 months or less, a person may choose hospice care. Hospice care is provided by a team of end-of-life care experts to alleviate suffering and provide support for the family.
Conclusion
James decided that home HD with his care partner was the best option for him as he begins an evaluation for a transplant. It is important for you to discuss the best treatment option for you with your healthcare team.
 Dr. Debra Hain has been a nephrology nurse for about 30 years starting as a dialysis nurse. In 2002 she became a nurse practitioner seeing patients in dialysis centers and conducting kidney disease education classes at Cleveland Clinic Florida, Department of Nephrology. In addition, she has her PhD in nursing and is an Associate Professor at Florida Atlantic University, Christine E. Lynn College of Nursing.
Dr. Debra Hain has been a nephrology nurse for about 30 years starting as a dialysis nurse. In 2002 she became a nurse practitioner seeing patients in dialysis centers and conducting kidney disease education classes at Cleveland Clinic Florida, Department of Nephrology. In addition, she has her PhD in nursing and is an Associate Professor at Florida Atlantic University, Christine E. Lynn College of Nursing.
Web ID 1061





 hemodialysis; 2) peritoneal dialysis; 3) kidney transplantation; or 4) palliative care.){kind=link}